














 29 / 52
29 / 52

Feb 2016
27
DISCUSSION
Ultraviolet light examination in a darkened room failed to
reveal fluorescence. Fluorescence under ultraviolet light is a
strong indication of dermatophytosis. Not all dermatophytes
fluoresce, but 60% of
Microsporum canis
lesions will
fluoresce. Circular scaling lesions such as these are often
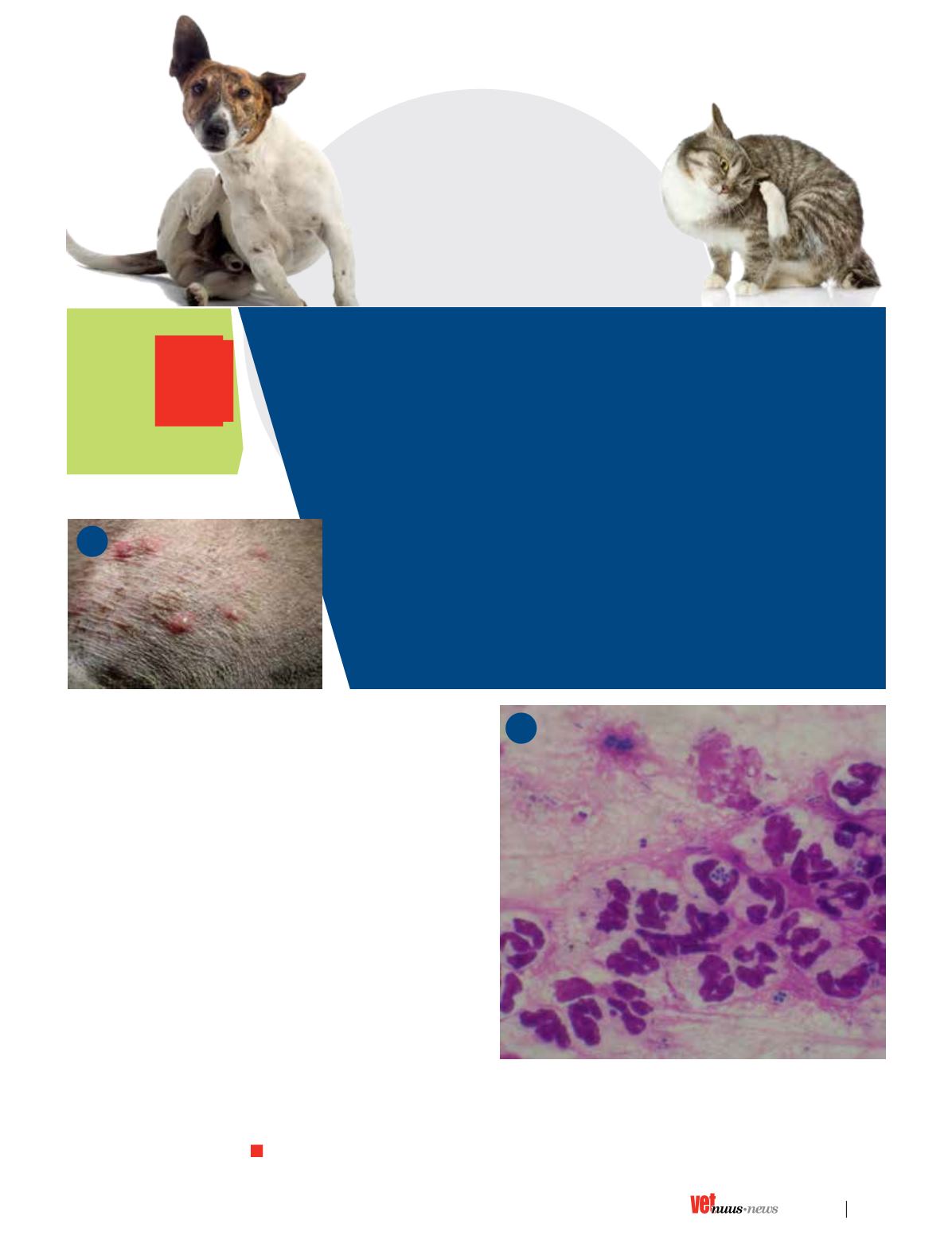
misdiagnosed as dermatophytosis. Careful removal of the
‘roof’ of an intact pustule and an impression smear stained
with Diff-Quick revealed numerous neutrophils (Figure 4).
Phagocytosed coccoid organisms are present in one of the
neutrophils – indicative of superficial pyoderma caused by
S. pseudintermediu
s. Cephalexin was prescribed at 20mg/kg
three times daily for 30 days. Prudence improved and was
maintained on a chlorhexidine-based shampoo and the coat
on the ventrum was kept short. The owners were cautioned
to examine Prudence for any developing pustules and apply
an antibiotic ointment effective against
S. pseudintermedius
(Mupirocin, Bactroban, GlaxoSmithKline) daily until
resolution.
There is a need to reduce evolutionary pressures which
encourage the growth of resistant strains, and at all times, the phenomenon of multidrug-resistant bacteria needs to be
kept in mind when prescribing antimicrobials. Although scientific evidence points to the use of antibiotics in man as the
most important factor promoting resistant strains, fluoroquinolones, macrolides and cephalosporins remain important
drugs in human medicine.
v
Dermatology Quiz
I Answers
4
Dermatology
Quiz
A
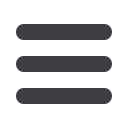
1. Circular scaling lesions or plaques are referred to as epidermal
collarettes. These circular lesions in Figures 1 and 2 have hyper-
pigmented centres.
2. Intact pustules (Figure 3).
3. Demodicosis, dermatophytosis, and other conditions characterized by
papules, pustules, and plaques, such as erythema multiforme, canine
eosinophilic dermatitis, superficial pyoderma, pemphigus foliaceus,
infectious dermatitides, adverse drug reactions, and toxic shock
syndrome
4. Ultraviolet light examination in a darkened room. Cytology of
an intact pustule stained with Diff-Quick stain for microscopic
examination under high power.
5. The primary treatment of superficial pyoderma is with appropriate
antibiotics for at least 21 and preferably 30 days. All clinical lesions
(except for complete regrowth of alopecic areas and resolution
of hyper-pigmented areas) should be resolved for at least 7 days
before antibiotics are discontinued. Antibiotics effective against
Staphylococcus pseudintermedius
should be selected.
3